
LEARNING METHOD AND MEDIUM
This educational activity consists of a written article and 20 study questions. The participant should, in order, read the Activity Description listed at the beginning of this activity, read the material, answer all questions in the post test, and then complete the Activity Evaluation/Credit Request form. To receive credit for this activity, please follow the instructions provided below in the section titled To Obtain CE Credit. This educational activity should take a maximum of 2 hours to complete.
CONTENT SOURCE
This continuing education (CE) activity captures key statistics and insights from contributing faculty.
ACTIVITY DESCRIPTION
This course is designed to help readers understand the development of the disease of myopia. The article identifies areas in which clinicians can intervene to slow progression using the latest research evidence from the past year.
TARGET AUDIENCE
This educational activity is intended for optometrists, contact lens specialists, and other eyecare professionals.
ACCREDITATION DESIGNATION STATEMENT
This course is COPE approved for 2 hours of CE credit. COPE Course ID: 102837-GO
DISCLOSURES
Cara Frasco Lai, OD, MS, is a consultant for Luminopia. Nicky Lai, OD, MS, has received honoraria from CooperVision.
DISCLOSURE ATTESTATION
The contributing faculty members have attested to the following:
1. That the relationships/affiliations noted will not bias or otherwise influence their involvement in this activity;
2. That practice recommendations given relevant to the companies with whom they have relationships/affiliations will be supported by the best available evidence or, absent evidence, will be consistent with generally accepted medical practice;
3. That all reasonable clinical alternatives will be discussed when making practice recommendations.
TO OBTAIN CE CREDIT
To obtain COPE CE credit for this activity, read the material in its entirety and consult referenced sources as necessary. We offer instant certificate processing for COPE credit. Please take the post test and evaluation online by using your OE tracker number and logging in to vccecredit.com.
Upon passing the test, you will immediately receive a printable PDF version of your course certificate for COPE credit. On the last day of the month, your course results will be forwarded to ARBO with your OE tracker number, and your records will be updated. You must score 70% or higher to receive credit for this activity. Please make sure that you complete the online post test and evaluation on a device that has printing capabilities.
NO-FEE CONTINUING EDUCATION
There are no fees for participating in and receiving credit for this CE activity.
Disclaimer
The views and opinions expressed in this educational activity are those of the faculty and do not necessarily represent the views of Contact Lens Spectrum. This activity is copyrighted to Conexiant ©2026. All rights reserved.
This activity is supported by an unrestricted educational grant from Contamac.
CE Questions? Contact accred@conexianteducation.com for help.
Release date: March 1, 2026
Expiration Date: February 28, 2029
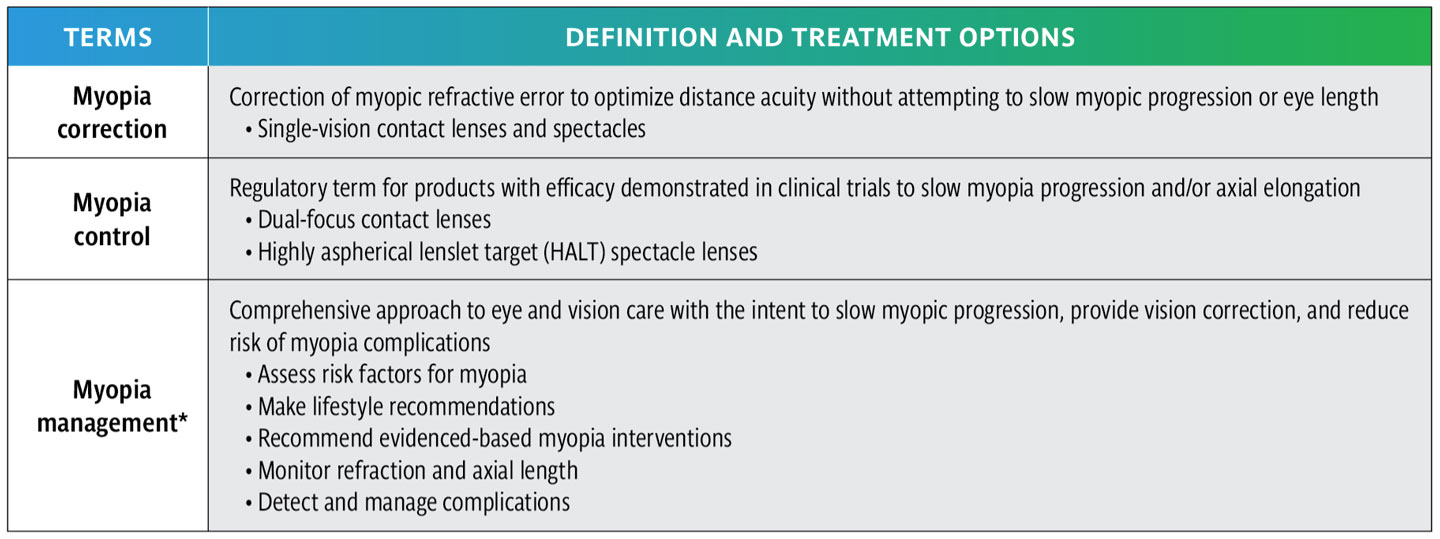
THIS IS AN EXCITING TIME, because myopia management—not just myopia correction—is the standard of care (Table 1).1 The US Food and Drug Administration (FDA) approval of a spectacle lens for myopia control in late 2025 equips all eyecare practitioners with tools for myopia management. This article goes beyond the basics of myopia management to provide eyecare practitioners with recent evidence-based information, providing insight on the potential mechanisms of myopic progression, reviewing available treatments, and reviewing the management of premyopia and high myopia.
Understanding the Disease to Optimize Treatment
Parental myopia and reduced time spent outdoors are risk factors for the development of myopia.2 Low hyperopic reserve and an accelerated rate of axial elongation are predictive factors that may indicate a child’s short-term risk of developing myopia.1
A comprehensive program of myopia management includes providing lifestyle recommendations to enhance retinal signaling and selecting evidence-based optical and/or pharmaceutical treatment to optimize retinal growth regulation. Emerging research reveals that early changes in choroidal thickness and retinal perfusion may indicate the efficacy of a treatment that protects the sclera from remodeling, which in turn could prevent axial elongation and myopic progression.1 In fact,a 1-year delay in the onset of myopia can lower the final level of myopia by 0.75 D for East Asian children, and 0.25 D to 0.50 D for non-East Asian children.3
Management of Premyopia
Although practitioners are greatly interested in slowing the progression of myopia in children who are already myopic, understanding the factors responsible for the onset of myopia may help to lessen the effects of myopia globally.
Hyperopic reserve: Low hyperopic reserve is the single greatest predictive factor for myopic progression.4 The Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) study, in an ethnically diverse sample, found that 6-year-old children who had less than +0.75 D were at increased risk for developing myopia by 8th grade and decreasing hyperopic reserve with age.3 Although only 3% to 5% of Chinese preschoolers are myopic, only 24% have age-appropriate hyperopic reserve.6 Chinese kindergarteners with a noncycloplegic refraction of >+0.70 D were found to have a low risk for becoming myopic by age 12, and those with >–0.70 D at low risk of high myopia.7
Based on findings of the CLEERE study, models were created that estimate the percentage of myopic children as a function of age, sex, and race/ethnicity. Axial elongation increases at a higher rate in younger ages and in Asian patients. An effective myopia management intervention could show a child shifting to a lower percentile with treatment.8
Retinal image and lifestyle recommendations: The mechanisms for slowing myopia progression are still under debate. The quality of the visual image and the intensity of light play roles in refractive development. Early research based upon animal models led to hypotheses that hyperopic defocus promotes myopic development and myopic defocus is protective.1 More recent research has found that peripheral defocus does not adequately explain the slowing of myopia progression achieved with soft multifocal contact lenses (MFCLs).9 Retinal exposure to light continues to be considered a possible mechanism for slowing myopia progression. Low lighting reduces the release of dopamine and favors signals leading to axial elongation.10
Time spent outdoors: Research has found that more time spent outdoors reduces the risk of myopia onset across a range of childhood ages.11 Despite this, the findings of the CLEERE study indicated that time outdoors and near work were not related to progression of myopia after a child became myopic.12 Later studies, however, have also found a reduction in myopia onset among children spending more time outdoors. And details such as the child’s current prescription and whether or not the parents are myopic are confounding factors that also seem to play a role in myopia onset.
Screen time: Near work and screen time have long been discussed as factors in the onset and progression of myopia; however, longitudinal studies have not found these factors to be predictive.11-13 Evaluating the relationship between screen time and the onset of myopia is complicated by the other factors mentioned in the previous paragraph.
Although some papers have shown that increased screen time can be associated with myopia, many analyses do not take these other factors into account.14-16 Additionally, it should be considered that those children who have higher amounts of screen time may be spending less time outdoors. Regardless, recommending that children spend less time using screens and more time outside and being physically active can only help ocular and systemic health.
Intervention for Premyopia
Children who are not myopic have been studied to determine whether any interventions can play a factor in preventing the disease. One study found that children who compliantly wore defocus-based spectacle lenses had a reduction in the 1-year incidence of myopia.17,18 Use of these spectacles only during near activities showed a slowing of refractive changes toward myopia by 54% (0.31 D) and axial elongation by 35% (0.12 mm) compared to controls.19
Use of 0.05% atropine nightly in a study of nonmyopic children found a reduction in the 2-year incidence of myopia from 53% to 28% and reduced myopic shifts of >–1.00 from 54% to 25% compared to the children given a placebo. Use of 0.01% atropine was not significantly better than a placebo in 4- to 9-year-old premyopes.20
Network meta-analysis shows that low-level red light therapy (0.48 D/year, 0.23 mm/year) and low-dose atropine (0.33 D/year, –0.12 mm/year) are the most effective interventions for reducing refractive progression and myopic incidence in East Asian children,21,22 however the safety of red light therapy has not been well studied in this population.
Pharmaceutical Interventions
The use of atropine emerged from theories that excessive accommodative effort resulted in myopia. Research now focuses on atropine’s action on growth regulatory transmission within the retina, choroid, and sclera.23,24 Atropine likely has direct and indirect effects on multiple receptors vs action on a single pathway. Alteration in the function of muscarinic, dopaminergic, alpha-2 adrenergic, and GABA receptors plays a role in the antimyopia effect of atropine.10,23,24
The Low-Concentration Atropine for Myopia Progression (LAMP) study found that concentrations of 0.05%, 0.025%, and 0.01% atropine were all effective in slowing the progression of myopia.25 Because the findings were found to be dose-dependent, the recommendation is to prescribe the highest concentration: 0.05% low-dose atropine. Clinically, if a child reports complaints such as photophobia or reading at near with this concentration, a lower concentration can be used.25 Another study found that East Asian children show the greatest response to dosages of atropine <0.1%.26 The highest rebound is also associated with atropine >0.1%, and tapering treatment is recommended when it is discontinued.27,28
Twice-daily vs once-daily dosing of 0.01% atropine slowed refractive progression by 53% (0.66 D vs 0.31 D) and axial elongation by 34% (0.21 mm vs 0.14 mm) in a 1-year study of Chinese children.29 The 0.5 mm increase in mesopic pupil diameter was not clinically significant. Children experiencing side effects while on a 0.05% dose may benefit from this novel dosing strategy.
Research has found that choroidal thickness and choroidal vessel volume as evaluated by OCT angiography are inversely related to axial length in children.30,31 One study found that 0.05% atropine induced the most pronounced increase in subfoveal choroidal thickness (25.70 µm), limited axial elongation (–0.21 mm), and myopic progression (0.54 D) compared to other atropine concentrations (0.1%, 0.01%, and 0.025%).32
Interestingly, attention-deficit/hyperactivity disorder (ADHD) is also associated with dopaminergic dysfunction. One study found that children who have untreated ADHD have a 1.2 times higher risk of myopia compared to peers without ADHD.33 Treatment with methylphenidate enhances dopamine signaling. Children taking this medication for ADHD showed a 39% reduced risk of myopia, and children taking multiple medications had additional protection.33
Optical Interventions
Optical interventions emerged from animal models showing that the type of blur (myopic or hyperopic) affects refractive development, with hyperopic defocus resulting in axial myopia.34-36 The goal of optical interventions is to differentially focus light on the central and peripheral retina to alter eye growth. Both spectacle and contact lens modalities offer “myopia correction” within a central optical zone for optimal distance visual acuity. Simultaneously, the devices alter the peripheral image through myopic defocus or, with newer applications, by altering peripheral image contrast.
Contact lens devices: Global fitting of contact lenses for myopia control has increased greatly over the past 13 years, with soft MFCLs making up 31% of soft lens fits and orthokeratology (ortho-k) lenses comprising 86% of all GP lens fits for children.37
Orthokeratology: Ortho-k effectively slows axial elongation and has high patient satisfaction with overall vision and quality of life compared to defocus spectacles.38 Predicting the ideal candidate and determining a given patient’s response to a myopia management intervention is vital.
Ortho-k effectiveness is less in younger patients and those who have lower levels of myopia.39 Parental education and commitment to follow-up appointments improves outcomes. Retrospective analysis of commercially available ortho-k designs reveals efficacy in controlling axial length and a low incidence of adverse events.40
To maximize the effectiveness of ortho-k for myopia management, consider selecting a lens design that has a smaller optic zone diameter (5.0 mm vs 6.0 mm), understanding that modifications to optic zone size may be needed because patients are more likely to show greater higher-order aberrations that can affect visual quality, depending on their pupil size.39,41,42
One study found that low myopes using ortho-k monotherapy were 2.2 times more likely to show fast (>0.20 mm/year) axial elongation, although adding 0.01% atropine significantly slowed elongation.43 When combining ortho-k and 0.01% atropine, instilling the drop in the morning lessens axial elongation (38%) more than evening dosing.44 There was no confounding effect on lens treatment zone or lens decentration, and no significant worsening of photophobia (9.4% to 12.8%).
A systematic review of rebound after discontinuation of myopia control treatment found a greater rebound response with ortho-k compared to soft MFCLs, although both modalities showed rebound. To lessen the rebound effect, it is recommended that children continue using ortho-k past 14 years of age.45 Those patients who wish to discontinue ortho-k may prefer MFCL wear due to the ease of lens care and maintenance, daytime wear, and stability of vision throughout the day.46
Soft multifocal lenses: Six years have passed since the FDA approved a dual-focus contact lens (DFCL) for myopia control and the Bifocal Lenses In Nearsighted Kids (BLINK) Study showed effectiveness of a +2.50 D center-distance soft MFCL.47,48 These technologies revolutionized clinical practice in the United States.
Many of those initial wearers are now adolescents, and optometrists may wonder whether these patients can now discontinue myopia management. Studies of these lenses found that older teenagers who stopped wearing a +2.50 D MFCL or a DFCL after 3 or 6 years did not show rebound and returned to age-normal myopic progression and axial elongation.49,50 Patients could benefit from MFCL use until elongation stops.49,50
As in other effective myopia treatments, BLINK Study subjects wearing +2.50 D add center-distance MFCLs showed increased choroidal thickness and area at 2 weeks compared to controls. This increase was maintained for 3 years and was associated with less axial elongation (0.23 mm).51
Spectacles: Although new to the United States in 2025, myopia management spectacles have been available globally for several years. As new designs become available, US eyecare practitioners benefit from robust evidence that the available lens designs slow myopic progression, and children do not show rebound when treatment ceases.52,53
Similar to contact lens modalities, spectacles offer vision correction within a central optical zone for optimal distance visual acuity. Simultaneously, the devices alter the peripheral retinal image through defocus-based mechanisms (Table 2).
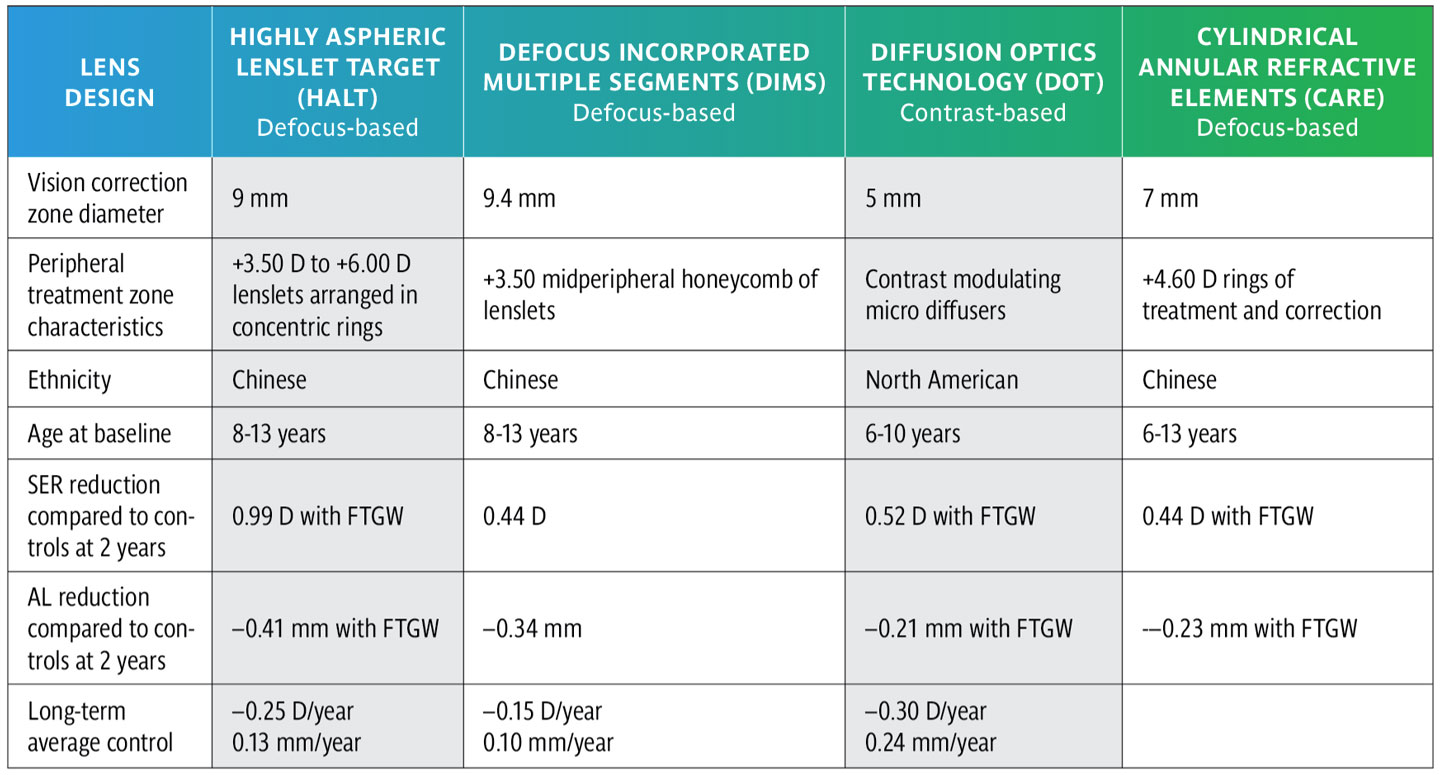
Contrast theory proposes that stimulation of the center-surround receptive field of retinal midget bipolar cells in the on/off retinal pathways signals contrast and regulates eye growth. The efficacy of defocus-based lenses may also be related to their alteration of retinal image contrast and image magnification vs myopia defocus.54-57 Studies of these spectacles show similar results.
Red Light
Red light therapy is the controversial use of a red light (650 nm) source for foveal viewing, which has not yet been proven to be safe for use in children and is not used in the United States. One study using red light therapy found reduced myopia incidence, slowed axial length elongation, and improved choroidal thickness and refraction in premyopes.61 Children using repeated low-level red light therapy for 1 year showed decreased cone density within 0.5 mm of the fovea and were 7.2 times more likely to show abnormal high-brightness signals near the fovea than controls.62 Red light therapy is not recommended at this time due to questions about the long-term safety and potential of rebound.62
Management of High Myopia
The effectiveness of slowing low to moderate myopia is well established. Because higher amounts of myopia are associated with greater sight-threatening complications, the possibility of slowing progression of myopia in children who already have high myopia is of great interest. Defocus-based spectacles and MFCLs (+2.50 D) effectively slow myopic progression in high myopes (–6.00 D to –10.00 D) compared to single-vision spectacles. MFCLs were shown to be more effective when used before the age of 12, although both treatments were equally effective after age 12.63 Adding a defocus-based spectacle lens to atropine (0.125%) in 6 to 15 year olds who have high myopia (<–6.00 D) further reduced progression and elongation.64
Participants in the BLINK2 Study were evaluated later as older adolescents, and 80% of the participants had some type of retinal finding, including: optic nerve crescent/pigmentation/peripapillary atrophy, white-without-pressure/dark-without-pressure, and retinal pigment epithelial hyper-/hypopigmentation; and 35% had a vitreous or peripheral finding that increases their risk for a future sight-threatening event.65 The presence of retinal abnormalities was not significantly associated with myopic progression or axial elongation.
Fundus tessellation (Figure 1) represents stage 1 myopic macular degeneration. Thinning of the retinal pigment epithelium and choroid heightens the visibility of the large choroidal vessels. Fundus tessellation is associated with decreased best-corrected acuity.66 A study of Chinese schoolchildren found that macular fundus tessellation patterns vs a peripapillary pattern was associated with longer axial length and high myopia.67 Children who did not have any tessellation had significantly shorter axial lengths. The density of tessellation and the area and width of peripapillary atrophy are associated with increasing risk of high myopia.68 Eyecare practitioners should note the presence and location of fundus tessellation, as this may identify a child at risk of myopia or in need of intervention.

Beyond 2026
Myopia is a multifactorial disease. As our understanding of the mechanisms involved improves, opportunities arise to intervene at multiple points in the process and monitor the eye’s response to treatment to maximize gains. Myopia management identifies risk and preventative factors (parental myopia and hyperopic reserve) and combines lifestyle recommendations (spending time outdoors daily, limiting screen, and near activities) with optical or pharmaceutical interventions. All children who have premyopia and myopia benefit from myopia management.69,70
References
1. Tahhan N, Bullimore MA, He X, et al. IMI-2025 digest. Invest Ophthalmol Vis Sci. 2025;66(12):27. doi: 10.1167/iovs.66.12.27
2. Morgan IG, Wu PC, Ostrin LA, et al. IMI risk factors for myopia. Invest Ophthalmol Vis Sci. 2021;62(5):3. doi: 10.1167/iovs.62.5.3
3. Bullimore MA, Brennan NA. Myopia: An ounce of prevention is worth a pound of cure. Ophthalmic Physiol Opt. 2023;43(1):116-121. doi: 10.1111/opo.13058
4. Zadnik K, Sinnott LT, Cotter SA, et al; Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) Study Group. Prediction of juvenile-onset myopia. JAMA Ophthalmol. 2015;133(6):683-689. doi: 10.1001/jamaophthalmol.2015.0471
5. Pu JN, Fang YX, Zhou Z, et al. The hyperopia reserve in 3-to 6-years-old preschool children in North China: the Beijing hyperopia reserve research. BMC Ophthalmol. 2025;25(1). doi: 10.1186/s12886-025-04008-9
6. Dong W, Fu KL, Zhang Y, et al. Hyperopic reserve as a predictor of myopia incidence in schoolchildren aged 6-12 years: a 24-month prospective cohort study. Front Public Health. 2025;13. doi: 10.3389/fpubh.2025.1660168
7. Mutti DO, Sinnott LT, Cotter SA, et al. Axial length as a function of age, sex, and ethnicity: Results from the CLEERE study. Optom Vis Sci. 2025;102(11):681-690. doi: 10.1097/OPX.0000000000002304
8. Lu Y, Yang X, Zhou J, et al. Diversified segmental defocus optimization lenses with and without atropine for myopia prevention: a randomized clinical trial. JAMA Ophthalmol. 2025;143(8):684-691. doi: 10.1001/jamaophthalmol.2025.2072
9. Berntsen DA, Ticak A, Sinnott LT, et al; BLINK Study Group. Peripheral defocus, pupil size, and axial eye growth in children wearing soft multifocal contact lenses in the BLINK Study. Invest Ophthalmol Vis Sci. 2023 Nov 1;64(14):3. doi: 10.1167/iovs.64.14.3
10. Yang Y, Lee D, Gettinger K, et al. Mechanisms underlying myopia progression from visual signaling to metabolic remodeling in retina. JMA J. 2025;8(4):1031-1038. doi: 10.31662/jmaj.2025-0268
11. Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci. 2007;48(8):3524-3532. doi: 10.1167/iovs.06-1118
12. Jones-Jordan LA, Sinnott LT, Cotter SA, et al; CLEERE Study Group. Time outdoors, visual activity, and myopia progression in juvenile-onset myopes. Invest Ophthalmol Vis Sci. 2012;53(11):7169-7175. doi: 10.1167/iovs.11-8336
13. Mutti DO, Mitchell GL, Moeschberger ML, Jones LA, Zadnik K. Parental myopia, near work, school achievement, and children’s refractive error. Invest Ophthalmol Vis Sci. 2002;43(12):3633-3640.
14. Ding H, Jiang L, Lin X, Ye C, Chun B. Association of physical activity, sedentary behaviour, sleep and myopia in children and adolescents: a systematic review and dose-response meta-analysis. BMC Public Health. 2025;25(1):1231. doi: 10.1186/s12889-025-22434-8
15. Xie S, He L, Xie X, Xu X. Effects of genetic factors and visual behaviors on interventions for myopia prevention and control in children: a systematic review and meta-analysis. Transl Pediatr. 2025;14(7):1602-1615. doi: 10.21037/tp-2025-409
16. Ha A, Lee YJ, Lee M, Shim SR, Kim YK. Digital screen time and myopia: a systematic review and dose-response meta-analysis. JAMA Netw Open. 2025;8(2):e2460026. doi: 10.1001/jamanetworkopen.2024.60026
17. Wang L, Wong YL, Drobe B, Wang X. Effectiveness of spectacle lenses with highly aspherical lenslets in slowing axial elongation among non-myopic children. Clin Exp Optom. 2025:1-7. doi: 10.1080/08164622.2025.2502527
18. Gao M, Hou Y, Lu Y, Shi Z, Zhao Q. Efficacy and safety of 0.01% atropine eye drops and novel lenslet-array-integrated spectacle lenses for the prevention of myopia progression among children with premyopia: a randomized clinical trial. Ophthalmol Ther. 2025;14(10):2481-2496. doi: 10.1007/s40123-025-01214-y
19. Ran G, Li X, Wen L, et al. Effectiveness of multizone-defocus-plano spectacles (MDPs) during nearwork in slowing axial elongation and myopic shift in non-myopic children: A cluster randomised controlled trial. Ophthalmic Physiol Opt. 2025;45(7):1935-1945. doi: 10.1111/opo.70023
20. Yam JC, Zhang XJ, Zhang Y, et al. Effect of low-concentration atropine eyedrops vs placebo on myopia incidence in children: The LAMP2 randomized clinical trial. JAMA. 2023;329(6):472-481. doi: 10.1001/jama.2022.24162
21. Lee SH, Tseng BY, Wang JH, Chiu CJ. Efficacy of myopia prevention in at-risk children: a systematic review and network meta-analysis. J Clin Med. 2025;14(5):1665. doi: 10.3390/jcm14051665
22. He M, Wang H, Du B, et al. 0.01% atropine for myopia prevention in pre-myopia (AMPP study). Ophthalmic Physiol Opt. 2025;45(7):1924-1934. doi: 10.1111/opo.70018
23. Horn D, Salzano AD, Jenewein EC, et al. Topical review: Potential mechanisms of atropine for myopia control. Optom Vis Sci. 2025;102(5):260-270. doi: 10.1097/OPX.0000000000002249
24. Upadhyay A, Beuerman RW. Biological mechanisms of atropine control of myopia. Eye Contact Lens. 2020;46(3):129-135. doi: 10.1097/ICL.0000000000000677
25. Yam JC, Jiang Y, Tang SM, et al. Low-concentration atropine for myopia progression (lamp) study: a randomized, double-blinded, placebo-controlled trial of 0.05%, 0.025%, and 0.01% atropine eye drops in myopia control. Ophthalmology. 2019;126(1):113-124. doi: 10.1016/j.ophtha.2018.05.029
26. Biswas S, Lanca C, Kynman-Sprinks D, Grzybowski A. Ethnic and dose-dependent differences in atropine efficacy for myopia control: a systematic review and meta-analysis. Br J Ophthalmol. 2025. doi: 10.1136/bjo-2025-328518
27. Chia A, Lu QS, Tan D. Five-year clinical trial on atropine for the treatment of myopia 2: myopia control with atropine 0.01% eyedrops. Ophthalmology. 2016;123(2):391-399. doi: 10.1016/j.ophtha.2015.07.004
28. Bullimore MA, Brennan NA. Efficacy in myopia control: the low-concentration atropine for myopia progression (LAMP) study. Ophthalmology. 2023;130(7):771-772. doi: 10.1016/j.ophtha.2023.02.020
29. He M, Zhang Z, Tong L, et al. Twice versus once daily application of 0.01% atropine for myopia control in children: a randomised controlled trial. Eye (Lond). 2025;39(17):3105-3112. doi: 10.1038/s41433-025-03964-2
30. Hiraoka T, Tamura M, Moriguchi Y, et al. Choroidal thickness distribution and its association with axial length and spherical equivalent in schoolchildren assessed by wide-field swept-source optical coherence tomography. Transl Vis Sci Technol. 2025;14(8):33. doi: 10.1167/tvst.14.8.33
31. Wu J, Wang N. Choroidal characteristics in 3- to 16-year-old chinese patients, measured by swept-source OCT/OCT angiography. Ophthalmol Sci. 2025;5(6):100869. doi: 10.1016/j.xops.2025.100869
32. Liu LP, Tang Y, Zhang JN, Du CX. Impact of atropine on changes in choroidal thickness in children with myopia: a meta-analysis of randomized controlled trials. Front Med (Lausanne). 2025;12:1678698. doi: 10.3389/fmed.2025.1678698
33. Huang YT, Lu JY, Tien PT, et al. Dopaminergic medications as a preventive for myopia: insights derived from pediatric patients diagnosed with attention deficit hyperactivity disorder. Postgrad Med J. 2025;101(1201):1127-1134. doi: 10.1093/postmj/qgaf051
34. Wildsoet C, Wallman J. Choroidal and scleral mechanisms of compensation for spectacle lenses in chicks. Vision Res. 1995 May;35(9):1175-94. doi: 10.1016/0042-6989(94)00233-c
35. Sivak JG, Barrie DL, Callender MG, Doughty MJ, Seltner RL, West JA. Optical causes of experimental myopia. Ciba Found Symp. 1990;155:160-172; discussion 172-177. doi: 10.1002/9780470514023.ch10
36. Hung LF, Crawford ML, Smith EL. Spectacle lenses alter eye growth and the refractive status of young monkeys. Nat Med. 1995 Aug;1(8):761-5. doi: 10.1038/nm0895-761
37. Efron N, Morgan PB, Woods CA, et al. International trends in prescribing contact lenses for myopia control (2011-2024): An update. Cont Lens Anterior Eye. 2025;48(5):102451. doi: 10.1016/j.clae.2025.102451
38. Li R, He X, Lin L, et al. Comparative study on the quality of life and clinical efficacy of orthokeratology lens, defocus spectacle lens and single vision spectacles in myopic children and adolescents in China. BMJ Open Ophthalmol. 2025;10(1):e002168. doi: 10.1136/bmjophth-2025-002168
39. Deng Y, Li X, Zhao M, Li Y, Wang K. Critical factors to predict efficacy of orthokeratology in inhibiting axial elongation in myopic children. BMC Ophthalmol. 2025;25(1):433. doi: 10.1186/s12886-025-04265-8
40. Xi W, Li H, Qi W, Tan T, Wang L. Long-term efficacy of crt, lucid, euclid, and ibright orthokeratology lenses in controlling myopia progression in children and adolescents: a 36-month retrospective cohort study. Clin Ophthalmol. 2025;19:2423-2430. doi: 10.2147/OPTH.S526689
41. Zamora-Castro C, Piñero DP, Martínez-Plaza E. Effect of optical zone diameter in orthokeratology on myopia control: a meta-analysis and systematic review. Eye Contact Lens. 2025;51(9):400-407. doi: 10.1097/ICL.0000000000001194
42. Sun M, Li M, Bi H, et al. Axial growth and meridian modulation of cornea power in children wearing orthokeratology lenses of different back optic zone diameters. Am J Ophthalmol. 2025;279:11-20. doi: 10.1016/j.ajo.2025.07.009
43. Fan Y, Li X, Chen S, Li Y, Zhao M, Wang K. Factors Influencing ortho-k treatment in low myopia and management approaches. Eye Contact Lens. 2025;51(9):386-393. doi: 10.1097/ICL.0000000000001208
44. Xiong ST, Li XW, Lu YC, Zhang MY, Li Y, Wang K. Morning administration is more effective than evening administration of 0.01% atropine eye drops combined with orthokeratology for myopia control. Indian J Ophthalmol. 2025;73(8):1153-1158. doi: 10.4103/IJO.IJO_3107_24
45. Chiu YC, Tsai PC, Lee SH, Wang JH, Chiu CJ. Systematic review of myopia progression after cessation of optical interventions for myopia control. J Clin Med. 2023;13(1). doi: 10.3390/jcm13010053
46. Cao Y, Liu J. Clinical advantages of multifocal soft contact lenses in myopia control for adolescents. Am J Transl Res. 2025;17(8):6009-6018. doi: 10.62347/ZURH1418
47. Chamberlain P, Peixoto-de-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year Randomized clinical trial of MiSight lenses for myopia control. Optom Vis Sci. 2019;96(8):556-567. doi: 10.1097/OPX.0000000000001410
48. Walline JJ, Walker MK, Mutti DO, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: the BLINK Randomized clinical trial. JAMA. 2020;324(6):571-580. doi: 10.1001/jama.2020.10834
49. Berntsen DA, Ticak A, Orr DJ, et al. Axial growth and myopia progression after discontinuing soft multifocal contact lens wear. JAMA Ophthalmol. 2025;143(2):155-162. doi: 10.1001/jamaophthalmol.2024.5885
50. Chamberlain P, Hammond DS, Bradley A, et al. Eye growth and myopia progression following cessation of myopia control therapy with a dual-focus soft contact lens. Optom Vis Sci. 2025;102(5):353-358. doi: 10.1097/OPX.0000000000002244
51. Walker MK, Berntsen DA, Robich ML, et al. Three-year change in subfoveal choroidal thickness and area with multifocal contact lens wear in the bifocal lenses in nearsighted kids (BLINK) study. Invest Ophthalmol Vis Sci. 2025;66(5):5. doi: 10.1167/iovs.66.5.5
52. D’Andrea L, Rinaldi M, Piscopo R, et al. Efficacy of spectacle lenses for myopia control: a meta-analysis of randomised controlled trials. Br J Ophthalmol. 2026 Jan 22;110(2):125-132. doi: 10.1136/bjo-2025-327629
53. Gupta V, Saxena R, Dhiman R, Phuljhele S, Sharma N. Comparative evaluation of different (peripheral defocus based) spectacle designs in preventing myopia progression: A double-blinded randomised clinical trial. Ophthalmic Physiol Opt. 2025;45(6):1505-1511. doi: 10.1111/opo.13548
54. Pons C, Mazade R, Jin J, Dul MW, Alonso JM. Optical defocus affects differently ON and OFF visual pathways. iScience. 2025;28(6):112500. doi: 10.1016/j.isci.2025.112500
55. Laughton D, Hill JS, McParland M, et al. Control of myopia using diffusion optics spectacle lenses: 4-year results of a multicentre randomised controlled, efficacy and safety study (CYPRESS). BMJ Open Ophthalmol. 2024;9(1). doi: 10.1136/bmjophth-2024-001790
56. Chalberg T, Laughton D, Hill J, et al. Control of myopia using diffusion optics spectacle lenses: efficacy and safety study (cypress) 42-month results. Invest Ophthalmol Vis Sci. 2023;64(8):5092-5092.
57. Neitz J, Neitz M. Diffusion optics technology (dot): a myopia control spectacle lens based on contrast theory. Transl Vis Sci Technol. 2024;13(10):42. doi: 10.1167/tvst.13.10.42
58. Bao J, Huang Y, Li X, et al. Spectacle lenses with aspherical lenslets for myopia control vs single-vision spectacle lenses: a randomized clinical trial. JAMA Ophthalmol. 2022;140(5):472-478. doi: 10.1001/jamaophthalmol.2022.0401
59. Lam CSY, Tang WC, Tse DY, et al. Defocus incorporated multiple segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020;104(3):363-368. doi: 10.1136/bjophthalmol-2018-313739
60. Chen X, Wu M, Yu C, et al. Efficacy of cylindrical annular refractive elements (CARE) spectacle lenses in slowing myopia progression over 2 years. Am J Ophthalmol. 2025;278:203-211. doi: 10.1016/j.ajo.2025.06.017
61. Leber MHM, Milbradt TL, Fujimura AY, Jr., et al. Effect of repeated intense foveal red-light therapy in children with pre-myopia: a systematic review and meta-analysis of randomized controlled trials. Curr Eye Res. 2025;50(11):1085-1093. doi: 10.1080/02713683.2025.2516007
62. Liao X, Yu J, Fan Y, et al. Cone density changes after repeated low-level red light treatment in children with myopia. JAMA Ophthalmol. 2025;143(6):480-488. doi: 10.1001/jamaophthalmol.2025.0835
63. Xiong R, Zhu Z, Jiang Y, et al. Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study. Clin Exp Ophthalmol. 2022 Dec;50(9):1013-1024. doi: 10.1111/ceo.14149
64. Li M, Zhang K, Hua B, et al. Multifocal contact lenses and defocus incorporated multiple segments lenses slow myopic progression in Chinese children with high myopia. J Optom. 2025;19(1):100588. doi: 10.1016/j.optom.2025.100588
65. Lee CY, Yang SF, Huang JY, Lian IB, Chang CK. The myopic control effect of defocus incorporated multiple segments’ spectacle lens with atropine in high myopia population. In Vivo. 2025;39(5):2950-2957. doi: 10.21873/invivo.14095
66. Schulle KL, Sinnott LT, Orr DJ, et al. Frequency of retinal findings after 8 years in the Bifocal Lenses in Nearsighted Kids (BLINK) Study. Ophthalmic Physiol Opt. 2025;45(6):1475-1484. doi: 10.1111/opo.13537
67. Jonas JB, Panda-Jonas S, Xu J, Wei WB, Wang YX. Associations of fundus tessellation, myopic diffuse chorioretinal atrophy and choroidal thickness with visual acuity in myopia. Acta Ophthalmol. 2025;103(8):1010-1019. doi: 10.1111/aos.17480.
68. Huang D, Lin X, Zhu H, et al. The associations between myopia and fundus tessellation in school children: a comparative analysis of macular and peripapillary regions using deep learning. Transl Vis Sci Technol. 2025;14(1):4. doi: 10.1167/tvst.14.1.4
69. Zou H, Liu J, Shi S, et al. Retinal features as predictive indicators for high myopia: insights from explainable multi-machine learning models. Front Bioeng Biotechnol. 2025;13:1609639. doi: 10.3389/fbioe.2025.1609639
70. Bullimore MA, Richdale K. Myopia cntrol 2020: where are we and where are we heading? Ophthalmic Physiol Opt. 2020;40(3):254-270. doi: 10.1111/opo.12686